
Achilles Tendonitis
In Vermont there is an abundance of runners who tough out the hilly roads and muddy trails year round, but there comes a time when even the some of the toughest runners around transition inside and onto a treadmill. Spending significant time on a treadmill sometimes leads to injury as there is an increased load on the Achilles tendon. 1 Another reason is that runners will tend to ‘mix it up’ more on a treadmill to keep from getting bored. This means more hill work, more speed work, etc. which can place the tendon under a new and different type of strain (eg. not the exact type of strain that it has adapted to absorb). 2
So, if you take to the treadmill a bit during crummy weather be on the look out, and try an ‘ounce of prevention’.
Who Gets it?
Achilles Tendonitis (AT) most commonly effects running athletes in their 30’s and 40’s. Males are affected more often than females accounting for 89% of all reported Achilles tendon injuries.
On average, 50% of runners will experience Achilles tendon pain at some point in their careers. And, for some, it can become a reoccurring nightmare.
What is it?
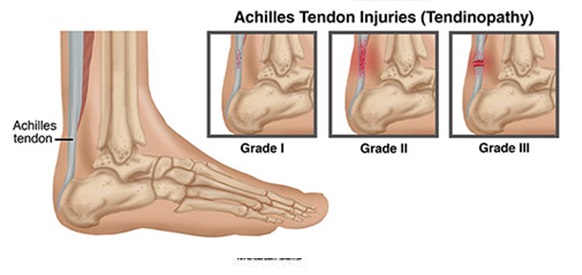
Achilles Tendonitis describes an irritation of the tendon along the back of the ankle that connects the calf muscles to the heel.

The AT is the thickest, strongest tendon in the body. The reason for this is that virtually all of the force generated when you “toe off” the ground during running is transmitted through the Achilles – and this force can be as much as three times your body weight!
‘Tendinopathy’ describes an accumulation of micro-damage that results when the demands placed on the tendon exceeds its functional capabilities:
LOAD X REPS > RECOVERY
Wear and tear builds up and the tendon may become inflamed (“Achilles Tendinitis”). Often, however, the tendon becomes dysfunctional with minimal inflammation – in these cases we see a ‘failed healing’ response and a gradual degeneration (not inflammation) of the tendon occurs. 3 For this reason, medical professionals will often refer to it as Achilles Tendinosis (remember ‘itis’ mean inflammation).
In short – the bodies’ natural healing mechanisms are unable to keep up with the daily wear – degeneration, micro-tearing and pain results.
The bulk of this blog is focused on chronic, overuse tendinosis; however, an Achilles injury can occur acutely. The severity of acute injuries is graded based on the amount of damage to the tendon:
https://www.youtube.com/watch?v=cgOemKqIzEE Here is an example of an ‘Acute’ injury in a world famous footballer David Beckham. He experiences a complete rupture of the Achilles tendon while playing for AC Milan in 2010. Obviously this ‘single episode’ acute injury more likely represents the culmination of sub-clinical trauma accumulation that weakens the tendon. How else can we explain a seemingly benign movement resulting in a torn tendon in a well-conditioned athlete? This injury happens in the very final minutes of the game – presumably fatigue plays a role as well. Beckham described afterwards that he had been training furiously to try and keep his spot on the English National Team for one last World Cup go. Failure to calculate appropriate recovery into training is a hallmark of this type of injury. Encouragingly – Beckham was able to return to the pitch (as a substitute) only 6 months after surgery. * Side note – watch Beckham’s reaction immediately after the injury. He turns and swings an arm behind him to swat the player that just kicked him… only, there’s no one there. Victims of Achilles tendon ruptures almost always report thinking that they were kicked (or shot!). |
What’s Happening?
As wear and tear builds up, and use overpowers recovery, the body’s healing and remodeling mechanisms are unable to maintain a healthy tendon. On a cellular level, what we see is that some of the collagen fibers are ruptured (If a tendon is a rope, think of collagen fibers as being the individual strands that make up the bulk of the rope). The body is able to lay down new fibers to replace the damaged ones, but it does so in a ‘disorganized’ way. These new fibers do not ‘align’ themselves properly and thus have limited ‘tensile’ strength.
A useful metaphor: Healthy Tendons – visualize a box of uncooked spaghetti noodles. All fibers are tightly packed together and lined up to resist forces in a single direction. This image is of a healthy tendon under a powerful microscope:
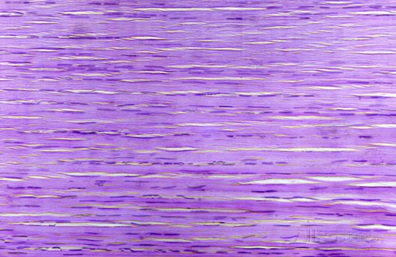
Unhealthy Tendons more closely resemble a bowl of cooked noodles. In the image below (which is of a damaged Achilles tendon) you can see the fibers are disorganized (not properly aligned in the plane of applied stresses) and not tightly packed together. This tissue is not ready to transfer tensile forces of 3 x your body weight!

What Does it Feel like?
The most common site to feel pain and stiffness is in the mid-portion of the tendon, just above the heel, although it may also present at the insertion onto the heel bone.
Early in the onset, the pain may be most obvious in the morning and at the beginning of activity (before getting properly ‘warmed up’). As the injury progresses, often the pain will be present towards the end of exercise (when fatigued) and/or after activity (when inflammation settles in).
The athlete may also experience increased calf muscle tension or a tendency to cramp. Additionally, there may be obvious swelling in the tendon, or at the insertion of the tendon onto the bone.
*** The ability of the athlete to ‘run through’ the pain initially often leads to a delay in seeking help. However, as we will see, treatment is more effective when caught early, so heed early warning signs. (David Beckham reported having very little awareness of pain/stiffness prior to his rupture… a ‘little’ pain and stiffness can indicate big problems on the horizon! ***
How to Diagnose it?
An accurate diagnosis is often possible in the office, and a proper clinical assessment can effectively rule out a tendon rupture. 4
Imaging techniques are often not needed to diagnose AT.
However, in difficult cases where the presentation is not completely clear, an MRI or Ultrasound may be helpful. 5
A evaluation with a sports physical therapist should include a thorough examination of the foot and ankle, a detailed movement assessment (e.g. your ability to walk/run, squat, stand on one leg, etc.) and an in-depth account of the injury onset and training history.
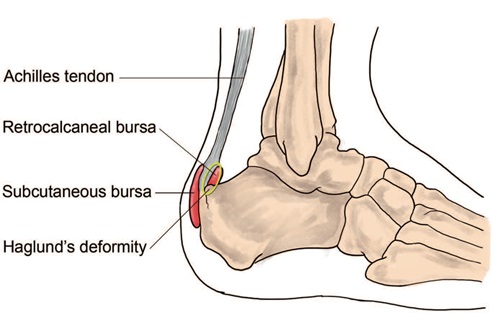
| Your Therapist will need to rule out other potential causes of posterior heel pain such as sural nerve entrapment/irritation, bursitis, and Posterior Ankle Impingement (PAI). PAI is often mis-diagnosed as ‘Insertional’ AT as it mimics many of the same symptoms. In this case, the pain and tissue damage is caused by compression of soft or bony tissue between the shin bone (tibia) and the heel bone (calcaneus). This can lead to inflammation in the tendon or the ‘Bursa’ sacs surrounding the tendon near the heel.
Some people have a small extra bone in the back of their ankle called the Os Trigonum that can lead to impingement. Also, small fragments of bone (i.e. bone chips) can break off the ankle bone and contribute to the development of an impingement syndrome. PAI may eventually lead to an Achilles Tendonopathy, but in these cases, the underlying cause, pathology and treatment strategy is different. For more information on posterior ankle impingement click here or here. |
What Causes it?
Achilles tendinopathy may result from a combination of several different variables, including:
- Ankle joint stiffness
- Calf muscle tightness
- Calf muscle weakness
- Abnormal foot structure
- Asymmetry in lower limb mechanics (when running)
- Improper footwear
- Training errors (*see below for examples)
What to do?
If you are beginning to feel symptoms of AT, be as proactive as possible. Remember, by the time you are feeling these symptoms, a sub-clinical accumulation of micro-trauma has likely been in place for weeks or months. It is not a new injury, it is simply an injury that has just recently reached the ‘tipping point’ and become symptomatic. Thus, it is unlikely to resolve on it’s own. If you rest it a bit, you may notice a resolution of symptoms. But, if you wish to return to prior training intensities, the underlying factors that contributed to the onset must be addressed.
Do not let symptoms linger unaddressed!
The longer the duration of symptoms, the more difficult the recovery.
| Some Basic Strategies to Try on Your Own Immediately
1) If you cannot walk quickly for at least 30 minutes (without a limp!) you should absolutely not be running. If your symptoms have reached this level of severity, some pro-active rest is necessary. Consult with a Sports Physical Therapist. 2) If you can walk longer distances, and run short distances without pain or limping, and you plan to continue running – reduce your weekly volume by 30-40%. 3) Warm up well! This may include a dynamic warm up, the use of non-impact machines (if running at the gym), or walking for 1-2 minutes and then transitioning to a running pace gradually. In the winter months, I’ve instructed outside runners to soak their legs in a hot bath / hot tub for 4-5 minutes just prior to running. The use of a compression sleeve to maintain muscle temperature after this type of ‘warm up’ can be helpful. * See Video for some ‘dynamic warm up’ strategies. 4) Start stretching your calfs – Some light / dynamic stretching pre-run and some longer static stretching post-run. * See Video 5) Start Foam rolling your calfs – This will decrease the muscle stiffness and allow for more efficient lengthening throughout your push off. 6) Avoid running on a road that is banked so that the center is raised relative to the sides (unless you can run down the center). Avoid training on a track and running in the same direction every session (this is especially important for indoor / short tracks). 7) Immediately stop any hill or speed work. 8) Increase your low-impact training – A spinning bike or Stairmaster are potentially good choices. Pool running is a great choice as well. 9) Consider your shoes – Have you recently made changes in shoe type? Both increasing or decreasing the amount of support (or stability) in the shoe can change the stresses placed on the AT. If you have not changed shoes in 4-6 months, perhaps it’s time. 300-400 miles may be the limit for one pair of shoes depending on body type and running style. (Best to consult with a Sports Medicine Professional familiar with running biomechanics for this one.) 10) Begin a training log. This should include daily information of training volume, intensity, and information on behavior of symptoms. A few weeks worth of this information can be very valuable to a Sports Medicine Professional counseling you on a proper recovery. |
Can this be Prevented?
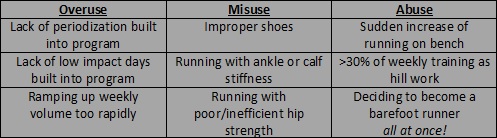
Yes. Like so many repetitive stress injuries, the onset of AT is related to overuse, misuse and/or abuse. See the table below to illustrate some potential contributing factors.
The most effective prevention strategy is to:
1) Have your training program / routine evaluated – For relatively new runners this means insuring that your progression of volume is not greater than 10% every 2 weeks. Additionally, your training days and rest days should be distributed appropriately throughout the week and your training ‘type’ (i.e. volume days vs. speed work or hills) needs to be appropriate for your experience level.
For more experienced or competitive runners this means calculating your acute:chronic training ratio and ensuring proper recovery strategies.
2) Have your gait evaluated – Get a running assessment by a sports Physical Therapist. This running assessment should include a video analysis of your running form (shoe and barefoot), a movement screen, and a detailed strength and mobility screen.
***** Recommendations on ‘Proper’ Running Form should be 100% individualized to the athlete based on body structure, injury history, training history, current gait mechanics and performance goals. Generic advice on ‘proper form’ that is distributed unselectively is not helpful… and may be harmful! *****
* Click here for more info on our Running Assessment – we offer the most detailed and professional screen in the region!
There are nearly countless potential variables that can increase strain at the Achilles Tendon and contribute to breakdown. Below are only a few examples to highlight the myriad factors that can contribute to the development of AT.
* Example – A runner with residual quad weakness after knee surgery who runs with a ‘peg leg’)
* Example – A runner with lateral hip weakness * Example – A runner transitioning to minimalist shoes too quickly * Example – A Runner compensating for poor forefoot alignment (may be in need of orthotics)
* Example – A runner with excessive ankle, hip or spine tightness
* Example – A runner forcing a transition to a forefoot strike pattern
* Example – A runner with past stress fracture in lateral foot * Example – A runner with poor balance * Example – A runner with SI joint instability |
What Physical Therapy Can Do?
Manual Therapy
Aggressive soft tissue mobilization to the calf and tendon can improve the mobility of the tissues 8 and facilitate recovery. 9
Decreased calf mobility has been identified as a risk factor for developing AT. 10
Instrument Assisted Soft Tissue Mobilization (IASTM) can be helpful as well. IASTM is a form of soft tissue manipulation that utilizes a tool to improve tissue mobility, break up adhesions, and stimulate your bodies innate healing mechanisms.
Animal Studies have shown that IASTM results in a quicker recovery from tendon injury, as well as a biomechanically stronger tendon after recovery. 11
Also, IASTM, when added to a comprehensive rehab program for AT, has been shown (in humans!) to provide added benefit – both short term and long term – including greater recovery of function. 12
Joint Mobilization may be indicated if motion restrictions in the foot or ankle are found to increase strain to the Achilles. 13 Mobilization of movement restrictions further up the ‘biomechanical chain’ may also be indicated. 14
Exercise Therapy
A properly tailored exercise program will take into consideration all evaluation findings and will often include:
1) Calf Strengthening. Weakness in the calf has be shown to be risk factor for developing AT. 15
2) Hip Strengthening. Hamstring weakness 16 and gluteal weakness 17 18 have been shown to contribute to the development of AT.
3) Core Strengthening. Dysfunctional Activation of the Transverse Abdominus muscle at specific moments during the gait cycle, has been demonstrated in runners with AT. 19
Also, Movement Re-Training Exercises can help to target specific gait dysfunction and improve gait efficiency. Research has demonstrated over and over again that isolated strengthening does not automatically translate into improved motor patterns (or improved running mechanics). A comprehensive rehabilitation strategy must include exercises specifically tailored to ‘re-educate’ proper movement.
Also, athletes with chronic AT have been found to have weaker Hip/Gluteal muscles when compared to their uninjured counterparts. 20
Eccentric Exercises
The exercise prescription should also include a graded progression of exercises prescribed to influence cellular level changes in the Achilles tendon. 21
This may include high-rep, low-rep exercises to increase circulation and improve lymph drainage. 22
Alternatively, this may include more aggressive ‘eccentric’ loading exercises for the more chronic/degenerative tendon. The goal of this type of intervention is to strengthen the tendon, reduce inter-tendon fluid retention / tendon thickness, and perhaps mitigate the negative effects of ‘neovasculization’ (the formation of microvascular networks that infiltrate a degenerative tendon and bring along nerve endings that may contribute to pain perception.) 23
* In patients with mid-tendon pain and swelling (the most common type of AT) a progressive eccentric loading program has been shown to be 90% effective * 24 25 26 27
Not only that, an aggressive eccentric exercise based approach has been shown to be effective even in chronic cases when other, more traditional (but ineffective!) approaches had failed.
Orthotics
A thorough evaluation of foot and ankle mechanics may lead to the recommendation for custom foot orthotics. Corrective orthotics may be indicated if:
1) Poor alignment of the foot, relative to the ankle, is found (a common finding in athletes with AT) 29 30
Orthotics are not necessary in most cases, but when needed, can help significantly.
Improving the foot stability through corrective orthotics can be effective at reducing pain 31 33 Also, orthotic therapy has been shown to improve the ‘load tolerance’ of Achilles Tendons in runners. 34
Corrective orthotics are a potentially effective adjunct to a comprehensive approach.
*** The Sports Physical Therapists at VASTA can fabricate custom orthotics if indicated.***
Other Interventions
- Low Level Laser Therapy (LLLT).
LLLT has been shown to have a positive effect on recovery from tendon injury. 35
With respect to AT specifically, some controlled studies have demonstrated reduced inflammation and decreased pain 36 as well as accelerated healing rates. 37 But, others studies have failed to demonstrate effectiveness. 38
There is certainly a theoretical model that supports it’s use as laboratory studies of LLLT has demonstrated a reduction of inflammation and an effectiveness equal to NSAIDS in animal studies. 39
While the research is not overwhelming, negative effects are limited and costs are minimal. LLLT can be used as an adjunct to a comprehensive approach to both acute and chronic AT.
- Heel Lifts
While a heel lift may be useful in cases of acute AT, where a proper gait pattern is difficult due to pain, the usefulness in Chronic cases appears to be minimal. 40 41
- Night Splints
Research into the effectiveness of night splints for AT is mixed. While some studies have shown a modest positive effect at reducing pain 42 others have demonstrated minimal effect.
For a patient who is compliant with a proper exercise based rehabilitation program, there appears to be no additional benefit to using a night splint. 43 44 Given that night splints are uncomfortable and often interrupt sleep (when the body is in ‘repair mode’), we typically do not recommend the use of night splints.
- Iontophoresis
Iontophoresis is the use of a medicated pad connected to an electric current to ‘drive’ the ionized medication into the tissue. Iontophoresis can be used to delivery a corticosteroid without injection. Compared to injection, it is safe, and without the risk of tendon rupture 45
Some studies have indicated a potential positive effect with Iontophoresis in patients with AT 46 but it appears to not be as effective in chronic cases.
Corrective Exercise, Manual Therapy and Training Modifications for Load Management are all part of a comprehensive rehabilitation plan.
It is important to give this time before considering other options – say, four to six months. This is due to 2 main considerations: 1) Tissue Response Time. Making training modifications and beginning interventions (like say, eccentric loading) in an attempt to positively effect tissues metabolism and micro-structure, is time dependent. It will take time for the cumulative effect of these changes to result in a healthier tendon and a meaningful reduction of pain; and 2) There isn’t convincing evidence that other options are any better. There are many more aggressive surgical and ‘alternative’ options out there. However, these are often expensive, sometimes very painful, may carry adverse side-effects and are not proven to be any more effective (and in many cases have been proven to be less effective) than the Physical Therapy approach described above.
For informational and decision making purposes, additional information is provided below regarding more invasive and ‘alternative’ options.
For patients looking for more information about minimally invasive and surgical interventions VASTA works in close communication with area Physician Specialists.
*** Talk to your Physical Therapist about setting up a referral ***
Additional Considerations
Acupuncture
The effectiveness of acupuncture in the treatment of AT is questionable as studies provide mixed results. Additionally, most studies that report some positive effect are, for the most part, of poor design and of very ‘low power’ (eg. single ‘case studies’ or non-controlled designs of small sample sizes), making it difficult to make meaningful recommendations.
Some recent research on Electro-Acupuncture has been interesting, 47 but certainly more research is needed as the ‘jump’ from animal studies to proving real significant improvement in humans beings is a big one.
* Recommendation – Not routinely recommended, but not necessarily discouraged (as an adjunct to rehabilitation) for patients who have had a positive response to acupuncture in the past.
Extracorporeal shock wave therapy (ESWT)
ESWT is the therapeutic use of abrupt, high amplitude pulses of mechanical energy, similar to soundwaves, generated by an electromagnetic coil. The research looking into the effectiveness of ESWT for AT has produced mixed results. Much of the research in support is not well controlled and overall the research supporting it’s use is unconvincing. 48
While some studies have shown a potential therapeutic effect, this is inconsistent. In addition, in studies that have demonstrated effectiveness, the therapeutic effect is no better than exercise therapy, 49 maybe less so. 50
* Recommendation – Not Recommended. It is expensive, and shown to be of no added benefit when compared to a proper rehabilitation approach.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDS)
NSAIDs, in addition to having multiple deleterious ‘side’ effects, have been shown to have minimal>no positive effect on recovery for patients with AT. 51 52
* Recommendation – Not Recommended.
Steroid Injections
The effectiveness of Corticosteroid Injections is questionable. Some studies have shown 53 short term pain relief, but likely at a cost of negative long-term effects including increased likelihood of recidivism, 54 and the proven adverse effect of delayed healing. 55
‘Peritendonous’ injections have been recently advocated as an adjunct to a proper, comprehensive conservative rehabilitation program due to less deleterious tendon weakening effects, 56 however, the positive effects remains somewhat equivocal. 57
* Recommendation – Direct Tendon Injections are not recommended. Peritendon Injections can be considered if the patient has failed to respond to an aggressive and comprehensive rehabilitation approach (4-6 months), and is determined to be a good candidate for this procedure.
Glyceryl Trinitrate (GTN) Patches
Also known as Nitroglycerine Patches, GTN is more commonly used to treat chest pain associated with heart disease. When Nitroglyercine is metabolized by your body it releases nitric oxide (NO) which, among other things, is a vasodilator (relaxing blood vessels and improving local blood flow).
NO has been shown in Laboratory studies to aid in Tendon healing (when your tendon is healthy, native NO levels are quite low, but when injured, its production is ramped up).
In theory GTN patches work by stimulating collagen synthesis (the type of fibers that make up a bulk of the AT). The research on GTN patches is somewhat mixed. Studies have determined a positive potential effect for tendonitis (in general), 58 and in patients with AT in particular 59 however, other studies looking specifically at AT have provided conflicting results 60 questioning it’s usefulness.
Some researchers also question the mechanism of effect in cases where a benefit is demonstrated. There is uncertainty whether the tendon healing effect of NO is real, or if the patch may simply act to temporarily decrease pain by increasing blood flow, but not provide any meaningful benefit to aid true structural healing and recovery. This is not a universally shared opinion. 61
Also, GTN patches also carry some concerns for adverse side effects, including severe headaches 62, and should be used with caution and always under the supervision of a medical provider.
* Reccommendation – Not recommended for widespread use. May be considered, under medical supervision, and as an adjunct to rehabilitation for patients who have failed to respond to an aggressive and comprehensive rehabilitation approach (4-6 months).
Sclerotherapy
Sclerotherapy involves injecting a chemical (typically polidocanol) into a blood vessel, which results in the sclerosis of that vessel. The reasoning behind using sclerotherapy for AT is based on the finding that there is a proliferation of small blood vessels in areas of chronic tendinopathy (see discussion of ‘neovascularization’ above). Importantly, small nerve endings appear to travel along with these new blood vessel formations. One theory is that these nerve fibers are a major pain generator in patients with AT. It is thought that the sclerosing therapy could not only destroy the vessels, but may also eradicate the pain-generating nerve fibers. A musculoskeletal specialist physician performs these injections under ultrasound guidance.
The research investigating sclerosing injections have shown some promise to reduce pain in more chronic cases that are unresponsive to conservative measures. 63 64 65
Although some studies suggest that polidocanol injections appear to provide pain relief, it is unclear what role they may play in promoting tendon healing. Other studies have failed to demonstrate improvement and specifically called into question prior studies claiming positive effects. 66
Last, and perhaps most importantly, long term studies must be done to demonstrate that the procedure is not ultimately detrimental to true healing. 67
* Recommendation – Not recommended for widespread use. The theory is intriguing, but more research must be done to demonstrate that this invasive technique provides added benefit over conservative approaches and does not weaken the tendon and expose it to future injury.
Prolotherapy
Prolotherapy is generically defined as an injection of an irritant solution (e.g. dextrose) into ligaments or tendon insertion in an effort to relieve pain and promote a local healing response. Overall Prolotherapy is a generic term with a wide range of meanings as the substance injected and the mode of injection can vary significantly.
For that reason, it is difficult to generalize about the data supporting or refuting it’s usefulness. With consideration of AT in particular, the research is mixed. Some studies have shown a positive effect (decreased pain levels and improved tendon ‘structure’) for patients with chronic AT. 68
Other studies, however, have shown only modest short-term improvements when compared to even a limited exercise-based rehabilitation program, with no added benefit seen in the long term.69
Also there is some potentially valid anecdotal concern that “prolotherapy injections may indeed help with protein synthesis and collagen formation… but (it may be) of (the) softer less dense Type III collagen which is formed rapidly and quickly after the injections, which for a stabilising ligament isn’t the best type… this excessive Type III collagen produced by prolotherapy injections may well actually prevent the formation of normal Type I collagen from being laid down with normal natural healing mechanisms, and so could cause potential long term deficits.” 70
* Recommendation – Not recommended for widespread use. Given the significant cost of the procedure (it is not covered by insurance), the painful nature of the procedure, and the questionable added benefit, it’s indication is uncertain. However, serious adverse side effects are very limited 71 with infection being the top concern. Thus, in some limited cases, where speed of recovery from a new injury is the top priority (eg. professional sports), prolothery could be considered, but the added benefit to an aggressive and comprehensive rehabilitation approach is questionable.
Platlet-rich Plasma (PRP) Injections
The material utilized in PRP injections is typically blood plasma with a high concentration of autologous (harvested from you) platelets. This PRP solution contains several different ‘growth factors’ and other ‘cytokines’ that are known to stimulate healing in soft tissues.
PRP injections are thus advocated as a ‘pro-regeneration’ intervention for damaged and degenerated tendons that have demonstrated a ‘failed healing’ response.
One issue with this theory, however, is that growth factors are already found in elevated concentrations in damaged tendons (even chronic injuries) as this appears to be one of your bodies natural responses to injury. Simply increasing these concentrations more is not a guarantee that the underlying imbalance of degeneration vs. regeneration will be corrected.
However, on a theoretical level, the potential of PRP and ‘regenerative medicine’ in general, is hugely attractive.
Researchers have attempted to investigate the potential effectiveness of PRP with controlled studies. As is almost always the case with a relatively new treatment approach, the initial results are mixed. 72
Despite a strong theoretical model of therapeutic potential, studies have generally failed to demonstrate that PRP injections are more beneficial than saline (placebo injection) in other types of Tendonopathy. 73 No strong evidence exists to suggest it’s usefulness in AT specifically. A recent review of research (a meta-analysis) of PRP use stated that current evidence suggests it “did not provide significantly greater clinical benefit versus placebo or dry needling for the treatment of tendinopathy.” 74
In spite of the limitations listed above, research into regenerative medicine is largely considered to be in it’s early stages. Additional studies are needed to determine the exact usefulness, optimal chemical compounding, optimal dosage, and optimal delivery. However, the potential for ‘regenerative medicine’ is largely considered to be substantial.
* Recommendation – Can be considered for patients who have been unresponsive (4-6 months) to an aggressive and comprehensive rehabilitation approach.
Stem Cell Therapy (SCT)
SCT largely fits under the umbrella of ‘regenerative medicine’ and is still fairly experimental. The basic idea behind this type of therapy is that stem cells can be delivered into an injury tissue (such as a degenerated tendon) and then triggered to differentiate into (turn into) into whatever cell type is needed to enhance the repair process.
While exciting potential exists for SCT, it shares many of the same challenges and questions as PRP treatments. Optimal Stem Cell type, concentration, and mode of delivery have not been well established; and the science demonstrating long term effectiveness and safety is limited. 75
* Recommendation – Not recommended for widespread use.
Surgery
Surgery is often considered an option of last resort in the treatment of AT. Surgical consideration should be saved for patients where pain persists after exhausting all conservative options.
Surgical Interventions for AT include “minimally invasive” procedures such as Percutaneous Needle Tenotomy (PNT). PNT is performed under ultrasound guidance (to identify the region of degeneration). A small needle is introduced into the damaged tendon region(s) and multiple ‘needlings’ are performed to cause micro-damage in an attempt stimulate a refreshed healing response.
PNT demonstrates reduces complications when compared to open surgical techniques, and it’s use does not preclude or otherwise hinder future surgical intervention if needed. 76
Overall, research demonstrating long-term effectiveness is still scarce, as this procedure is relatively new. One study of PNT for AT patients reported a ~ 75% success rate 77 (but keep in mind this is the ‘fairly good’ recovery rate after 18 months!).
An open surgical debridement (“cleaning up”) is another more invasive (compared to PNT) option. The effectiveness of a surgical debridement for AT appears to be dependent on the extent of damage present. 78
One study of patients with chronic paratendonitis who underwent surgical debridement reported a ‘good’ (or better) success rate ~ 85% of the time. 79
In this same study, patients with true tendon degeneration experienced less encouraging results (‘satisfactory’ results or better ~ 65% of the time).
* Keep in mind! The research definition of ‘good’ or ‘satisfactory’ is rarely what I hear my patients saying they are looking for as an outcome! (eg. it ain’t running pain-free).
Open surgical ‘removal of pathology’ is typically a last resort. Published “success” rates for pain reduction are ~ 80%. The ability of open surgery to improve function again depends on the extent of tissue impairment. With success rates for patients with marked “intratendinous lesion(s)” reported as 54%. 80

This image shows an open ‘repair’ of an achilles tendon. Note the central degenerated section within the tendon.
* Keep in mind! ‘Success’ was defined as a recovery of function. This improved function is typically tested with somewhat easy tasks such as stair climbing and heel raises – not sprinting, jumping, etc.
Also, of interest, a recent review of research has demonstrated that ‘success rates’ published have been worsening over that past few decades (despite advances in surgical techniques). This is believed to be a result of improved research methods demonstrating more realistic reporting. 81 82
* Recommendation – All surgical approaches are to be avoided unless absolutely necessary! We are lucky to live in an area with highly skilled surgeons. Should we need their services, we are grateful for their help… but, we should be working hard to NOT seek their help (and they would encourage that!)
For patients looking for more information about minimally invasive and surgical interventions VASTA works in close communication with area Physician Specialists.
*** Talk to your Physical Therapist about setting up a consultation ***
- Willy, R.; et al. Patellofemoral Joint and Achilles Tendon Loads During Overground and Treadmill Running. J of Ortho & Sports PT . 2016; 46; 664-72. “...treadmill running resulted in greater Achilles tendon loading compared with overground running.“
- Gottschall JS, Kram R. Ground reaction forces during downhill and uphill running. J Biomech. 2005 Mar;38(3):445-52. “…Combined with previous biomechanics studies, our normal impact force data suggest that downhill running substantially increases the probability of overuse running injury. Our parallel force data provide insight into past energetic studies, which show that the metabolic cost increases during downhill running at steep angles.”
- Khan KM, Cook JL, Bonar F, Harcourt P, Astrom M. Histoathology of common tendinopathies. Update and implications for clinical management. Sports Med. 1999 Jun;27(6):393-408. Often, there is an abrupt discontinuity of both vascular and myofibroblastic proliferation immediately adjacent to the area of greatest abnormality. The most significant feature is the absnce of inflammatory cells. These observations confirm that the histopathological findings in athletes with overuse tendinopathies are consistent with those in tendinosis…”
- Maffulli N. The clinical diagnosis of subcutaneous tear of the Achilles tendon. A prospective study in 174 patients. Am J Sports Med. 1998 Mar-Arp;26(2):266-70. “Both the calf squeeze and Matles tests were significantly more sensitive than the other tests…. the tests showed a high capability to detect that the Achilles tendon was intact.”
- Alfredson H, Cook J. A treatment algorithm for managing Achilles tendinopathy: new treatment options. Br J Sports Med. 2007 Apr;41(4):211-216. “…if a clinical diagnosis is not clear, ultrasonography or MRI may reveal the pathology with in the tendon….”
- Azevedo LB, et al. Biomechanical variables associated with Achilles tendinopathy in runners. Br J Sports Med. 2009 Apr;43(4):288-92) “…Altered knee kinematics and reduced muscle activit are associated with Achilles tendinopathy in runners. Rehabilitation exercises or other mechanisms (e.g. footware) that affect kinematics and muscle activity may therefore be beneficial in the treatment of runners with Achilles tendinopathy.”
- Ryan, M., Grau, S., Krauss, I., Maiwald, C., Taunton, J., & Horstmann, T. (2009). Kinematic Analysis of Runners with Achilles Mid-Portion Tendinopathy. Foot and Ankle International, 30(12), 1190–1195 “…we found an increase in eversion displacement of the sub-talar joint in runners with Achilles mid-portion tendinopathy.”
- Carcia C, Martin R, Houck J, Wukich D. Achilles pain,m stiffness, and muscle power deficits: achilles tendinitis. J Orthop Sports Phys Ther. 2010:40(9):A1-A26.
- Alfredson H, Cook J. A treatment algorithm for managing Achilles tendinopathy: new treatment options. Br J Sports Med. 2007 Apr;41(4):211-216. “…if a clinical diagnosis is not clear, ultrasonography or MRI may reveal the pathology with in the tendon….“
- Kaufman KR, et al. The effect of foot structure and range of motion on musculoskeletal overuse injuries. Am J Sports Med. 1999 Sept-Oct;27(5):585-93. “The subjects were tracked prospectively for injuries throughout training. We identified risk factors that predispose people to lower extremity overuse injuries. These risk factors include dynamic pes planus, pes cavus, restricted ankle dorsiflexion, and increased hindfoot inversion, all of which are subject to intervention and possible correction.”
- Imai K, et al. Tissue Mobilization Therapy on Achilles Tendinopathy in a Rabbit Model. Feb, 28(2)112-8. “…Biomechanical and histological findings showed that the Achilles tendons treated with ASTM had better recovery of biomechanical function that did control tendons.”
- McCormack JR, et al. Eccentric Exercise Versus Eccentric Exercise and Soft Tissue Treatment (Astym) in the Management of Insertional Achilles Tendinopathy: A Randomized Controlled Trial. Sports Health. 2016 Feb. “…Soft tissue treatment (Astym) plus eccentric exercise was more effective than eccentric exercise only at improving function during both short- and long-term follow-up periods.”
- Kaufman KR, et al. The effect of foot structure and range of motion on musculoskeletal overuse injuries. Am J Sports Med. 1999 Sept-Oct;27(5):585-93. “The subjects were tracked prospectively for injuries throughout training. We identified risk factors that predispose people to lower extremity overuse injuries. These risk factors include dynamic pes planus, pes cavus, restricted ankle dorsiflexion, and increased hindfoot inversion, all of which are subject to intervention and possible correction.”
- Voorn R. Case report: can sacroiliac joint dysfunction cause chronic Achilles tendinitis? J Orthop Sports Phys Ther. 1998 Jun;27(6):436-43.
- Mahieu NN, et al. Intrinsic risk factors for the development of achilles tendon overuse injury: a prospective study. Am J Sports Med. 2006 Feb;34(2):226-35. “…the strength of the plantar flexors and amount of dorsiflexion excursion were identified as significant predictors of an Achilles tendon overuse injury. A plantar flexor strength lower than 50.0 N.m and dorsiflexion range of motion higher than 9.0 degrees were possible thresholds for developing an Achilles tendon overuse injury.”
- Hein T, et al. Prospective analysis of intrinsic and extrinsic risk factors on the development of Achilles tendon pain in runners. Scandinavian J Med & Sci in Sports. June 2014 (3)e201-12. “…runners developing Achilles tendon pain already show differences in their lower extremity kinematics, muscular strength, and training habits. More extended knee and ankle joints lead to a more forward-shifted touchdown and higher stress on the Achilles tendon during the weight bearing”
- Franettovich Smith MM, et al. Neuromotor control of gluteal muscles in runners with achilles tendinopathy. Med Sci Sports Excerc. 2014 Mar;46(3):594-9. “…This study provides preliminary evidence of altered neuromotor control of the GMED and GMAX muscles in male runners with Achilles tendinopathy. Although further prospective studies are required to discern the causal nature of this relationship, this study highlights the importance of considering neuromotor control of the gluteal muscles in the assessment and management of patients with Achilles tendinopathy.”
- Azevedo LB, et al. Biomechanical variables associated with Achilles tendinopathy in runners. Br J Sports Med. 2009 Apr;43(4):288-92) “…Altered knee kinematics and reduced muscle activit are associated with Achilles tendinopathy in runners. Rehabilitation exercises or other mechanisms (e.g. footware) that affect kinematics and muscle activity may therefore be beneficial in the treatment of runners with Achilles tendinopathy.”
- Azevedo LB, et al. Biomechanical variables associated with Achilles tendinopathy in runners. Br J Sports Med. 2009 Apr;43(4):288-92) “…Altered knee kinematics and reduced muscle activit are associated with Achilles tendinopathy in runners. Rehabilitation exercises or other mechanisms (e.g. footware) that affect kinematics and muscle activity may therefore be beneficial in the treatment of runners with Achilles tendinopathy.”
- Habets B, Smits HW, Backx FJG, van Cingel REH, Huisstede BMA. Hip muscle strength is decreased in middle-aged recreational male athletes with midportion Achilles tendionapthy: A cross-sectional study. Phys Ther in Sport. 2017 May;25:55-61. “Compared to controls, participants with AT demonstrated 28.9% less isometric hip abduction strength (p = 0.012), 34.2% less hip external rotation strength (p = 0.010), and 28.3% less hip extension strength (p = 0.034) in the injured limb.”
- Ohberg L, Lorentzon R, Alfredson H. Eccentric training in patients with chronic Achilles teninosis: normalised tendon structure and decreased thickness at follow up. Br J Sports Med. 2004;38:8-11. “…Ultrasonographic follow up of patients with mid-portion painful chronic Achilles tendinosis treated with eccentric calf muscle training showed a localised decrease in tendon thickness and a normalised tendon structure in most patients. Remaining structural tendon abnormalities seemed to be associated with residual pain in the tendon.”
- Torstensen T, Meen H, Stiris M. The effect of medical exercise therapy on a patient with chronic supraspinatus tendinitis. Diagnostic ulatrasound-tissue regeneration: a case study. J Of Ortho & Sports Phys Ther. 1994;20(6)319-27.
- O’Neill S, Watson P, Barry S. Why are eccentric exercises effective for achilles tendinopathy? Int J Sports Phys Ther. 2015 Aug;10(4):552-62.
- Alfredson H, et al. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998 May-Jun;26(3):360-6.
- Fahlstrom M, et al. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc. 2003 Sep;11(5):327-33.
- Roos EM, et al. Clinical improvement after 6 weeks of eccentric exercise in patients with mid-portion Achilles tendinopathy–a randomized trial with 1-year follow-up. Scand J Med Sci Sports. 2004 Oct;14(5):286-95.
- Gardin A, et al. The long-term clinical and MRI results following eccentric calf muscle training in chronic Achilles tendinosis. Skeletal Radiol. 2010 May;39(5):435-42.
- Kvist M. Achilles tendon injuries in athletes. Ann Chir Gynaecol. 1991;80(2):188-201. “…Different structural faults were found in 60% of the athletes with Achilles tendon overuse injuries. Forefoot varus correlated (r = P less than 0.001) with paratenonitis.”[/note]; or
2) The gait assessment reveals grossly excessive pronation – which has been linked to the development of AT by multiple studies. 28McCrory JL, et al. Etiologic factors associated with Achilles tendinitis in runners. Med Sci Sports Exerc. 1999 Oct;31(10):1374-81.“…arch index were found to be significant discriminators…between runners afflicted with Achilles tendinitis and runners who had no history of overuse injury.“
- Reule CA, et al. Spatial orientation of the subtalar joint axis is different in subjects with and without Achilles tendon disorders. Br J Sports Med. 2011 Oct;45(13):1029-34. “…the mean deviation angle (of the ankle joint) in people with Achilles tendon pathologies is significantly more oblique than in people without. This finding indicates that the spatial orientation of the (ankle joint) is related to the incidence of overuse injuries of the Achilles tendon in the investigated sample” (long-distance runners)
- Mayer F, et al. Effects of short-term treatment strategies over 4 weeks in Achilles tendinopathy. Br J Sports Med. 2007 Jul;41(7):e6. “...Most patients with AT experience a reduction in pain after only 4 weeks of differentiated, non-surgical treatment consisting of physiotherapy or semi-rigid insoles.”
- Donoghue OA, et al. Orthotic control of rear foot and lower limb motion during running in participants with chronic Achilles tendon injury. Sports Biomech. 2008 May;7(2):194-205. “…participants reported between 50 and 100% (average 92%) relief from symptoms with the use of orthoses.”[/note] and altering neuromuscular recruitment patterns of the calf muscles (which may be dysfunctional in runners with chronic AT). 32Wyndow N, et al. Neuromotor control of the lower limb in Achilles tendinopathy: implications for foot orthotic therapy. Sports Med. 2010 Sep 1;40(9):715-27. “…it is possible that foot orthoses may aid to normalize intratendinous loads via altering neuromotor activity in the triceps surae (calf muscle) in AT.”
- Sinclair J, Isherwood J, Taylor PJ. Effects of foot orthoses on Achilles tendon load in recreational runners. Clinical Biomech, 2014 Sept;29(8):956-8. “…The results indicate that running with foot orthotics was associated with significant reductions in Achilles tendon load compared to without orthotics… the current investigation suggests that via reductions in Achilles tendon load, foot orthoses may serve to reduce the incidence of chronic Achilles tendon pathologies in runners.”
- Tumilty S, et al. Low level laser treatment of tendinopathy: a systematic review with meta-analysis. Photomed Laser Surg. 2010 Feb;28(1):3-16. “…LLLT can potentially be effective in treating tendinopathy when recommended dosages are used. The 12 positive studies provide strong evidence that positive outcomes are associated with the use of current dosage recommendations for the treatment of tendinopathy.”
- Bjordal JM, Lopes-Martins RA, Iversen VV. A radomised, placebo controlled trial of low level laser therapy for activated Achilles tendinitis with microdialysis measurement of peritendinous prostaglandin E2 concentrations. Br J Sports Med. 2006 Jan;40(1):76-80. “LLLT at a dose of 5.4 J per point can reduce inflammation and pain in activated Achilles tendinitis.”
- Stergioulas A, et al. Effects of low-level laser therapy and eccentric exercises in the treatment of recreational athletes with chronic achilles tendinopathy. Am J Sports Med. 2008 May;36(5):881-7. “…Low-level laser therapy, with the parameters used in this study, accelerates clinical recovery from chronic Achilles tendinopathy when added to an EE regimen. For the LLLT group, the results at 4 weeks were similar to the placebo LLLT group results after 12 weeks.”
- Tumilty S, et al. Clinical effectiveness of low-level laser therapy as an adjunct to eccentric exercise for the treatment of Achilles’ tendinopathy: a randomized controlled trial. Arch Phys Med Rehabil. 2012 May;93(5):733-9. “…The clinical effectiveness of adding LLLT to eccentric exercises for the treatment of Achilles’ tendinopathy has not been demonstrated using the parameters in this study.”
- Bjordal J, et al. The anti-inflammatory mechanism of low level laser therapy and its relevance for clinical use in physiotherapy. J Phys Ther Rev 2013 Jul;15(4):286-93. “…Red and near infrared LLLT administered with mean laser output of 2.5–100 mW, irradiation times of 16–600 s and doses of 0.6–9.6 J reduces inflammation significantly, and is equally effective as NSAIDs in animal laboratory studies. “
- MacLellan GE, Vyvyan B. Management of pain beneath the heel and Achilles tendonitis with visco-elastic heel inserts. Br J Sports Med. 1981 Jun;15(2):117-21.
- Lowdon A, Bader DL, Mowat AG. The effect of heel pads on the treatment of Achilles tendinitis: a double blind trial. Am J Sports Med. 1984 Nov-Dec;12(6):431-5. “…the claimed benefit of viscoelastic pads widely used by athletes was not substantiated”
- Roos EM, et al. Clinical improvement after 6 weeks of eccentric exercise in patients with mid-portion Achilles tendinopathy–a randomized trial with 1-year follow-up. Scand J Med Sci Sports. 2004 Oct;14(5):286-95. “…the claimed benefit of viscoelastic pads widely used by athletes was not substantiated”
- de Vos RJ, et al. The additional value of a night splint to eccentric exercises in chronic midportion Achilles tendinopathy: a randomised controlled trial. Br J Sports Med. 2007 Jul;41(7):e5. “…A night splint is not beneficial in addition to eccentric exercises in the treatment of chronic midportion Achilles tendinopathy.“
- Petersen W, Welp R, Rosenbaum D. Chronic Achilles teninopathy: a prospective randomized study comparing the therapeutic effect of eccentric training, the AirHeel brace, and a combination of both. Am J Sports Med. 2007 Oct;35(10):1659-67. “…The AirHeel brace is as effective as eccentric training in the treatment of chronic Achilles tendinopathy. There is no synergistic effect when both treatment strategies are combined.”
- Brown D, Lauber CA. Evidence based guidelines for utilisation of dexamethasone iontophoresis. Internat J Athl Ther Training. 2011;16(4):33‐36.
- Neeter C, et al. Iontophoresis with or without dexamethazone in the treatment of acute Achilles tendon pain. Scand J Med & Sci in Sports. 2003 Dec;13(6):376-82. “…positive effects from using iontophoresis with dexamethazone were found in the treatment of patients with acute Achilles tendon pain.”
- Inoue M, et al. The effect of electroacupuncture on tendon repair in a rat Achilles tendon rupture model. Acupunct Med. 2015 Feb;33(1):58-64. “…The marked increase in cell count and growth factor expression as well as increased tendon strength in the EA group suggest that EA may be a useful method for promoting tendon repair.”
- Andres M, Murrell G. Treatment of Tendinopathy: What works, what does not, and what is on the horizon. Clin Orthop Relat Res. 2008 Jul;466(7):1539-54.” This treatment modality has been extensively studied over the past 10 years, and there is a great deal of variability in the data…Further evidence is needed to justify the use of ESWT in Achilles tendinopathy and patellar tendinopathy.”
- Rompe JD, Nafe B, Furia JP, Maffulli N. Eccentric loading, shock-wave treatment, or a wait-and-see policy for tendinopathy of the main body of tendo Achillis: a radomized controlled trial. Am J Sports Med. 2007 Mar;35(3):374-83.
- Magnussen RA, Dunn WR, Thomson AB. Nonoperative treatment of midportion Achilles tendinopathy: a systematic review. Clin J Sport Med. 2009 Jan 19(1):54-64.
- Astrom M, Westlin N. No effect of piroxicam on achilles tendinopathy. A randomized study of 70 patients. Acta Orthop Scand. 1992 Dec;63(6):631-4. “…No differences were seen between the groups at any time during the study.”
- McLauchlan GJ, Handoll HH. Interventions for treating acute and chronic Achilles tendinitis. Cochrane Database Syst Rev. 2001;(2):CD000232. “…There was weak but not robust evidence from three trials of a modest benefit of NSAIDs for the alleviation of acute symptoms… The results of a comparison of glycosaminoglycan sulfate with a NSAID were inconclusive.”
- Almekinders LC, Temple JD. Etiology, diagnosis, and treatement of tendonitis: an analysis of the literature. Med Sci Sports Exerc. 1998 Aug;30(8):1183-90. “…Twenty-three studies on steroid injections were found. Eight were prospective and placebo controlled studies, with three showing beneficial effects of the injection at follow-up. It was concluded that much of the pathology and etiology of tendonitis remains unclear.”
- Smidt N, et al. Corticosteroid injections, physiotherapy, or a wait-and see policy for lateral epicondylitis: a randomised controlled trial. Lancet. 2001 Feb 23;359(9307):657-62.
- Fredberg U. Local corticosteroid injection in sport: review of literature and guidelines for treatment. Scand J Med Sci Sports. 1997 Jun;7(3):131-9. “Injection of corticosteroid inside the tendon has a deleterious effect on the tendon tissue and should be unanimously condemned.”
- Gill SS, et al. Fluoroscopicallly guided low-volume peritendinous corticosteroid injection for Achilles tendinopathy. A safety study. J Bone Joint Surg Am. 2004 Apr;86-A(4):802-6. “This… study establishes the safety of low-volume injections of corticosteroids for the treatment of Achilles tendinopathy when the needle is carefully inserted into the peritendinous space under direct fluoroscopic visualization.”
- Shrier I, Matheson GO, Hohl HW 3rd. Achilles tendonitis: are corticosteroid injections useful or harmful? Clin J Sport Med. 1996 Oct;6(4):245-50. “There are insufficient published data to determine the comparative risks and benefits of corticosteroid injections in Achilles tendonitis. The decreased tendon strength with intratendinous injections in animal studies suggests that rupture may be a potential complication for several weeks following injection.”
- Gambito Ed, et al. Evidence on the effectivenss of topical nitroglycerin in the treatment of tendinopathies: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2010 Aug;91(8):1291-305. “In chronic tendinopathies, there is strong evidence for NTG in relieving pain during activities of daily living, and increasing tendon strength. Further studies are needed to explore the role of this promising intervention in all phases of tendinopathies.”
- Paoloni JA, et al. Topical glyceryl trinitrate treatment of chronic noninsertional achilles tendnopathy. A randomized double-blind, placebo-controlled trial. J Bone Joint Surg Am. 2004 May;86-A(5):916-22. “Topical glyceryl trinitrate significantly reduced pain with activity and at night, improved functional measures, and improved outcomes in patients with Achilles tendinopathy.”
- Kane TP, Ismail M, Calder JD. Topical glyceryl trinitrate and noninsertional Achilles tendinopathy: a clinical and cellular investigation. Am J Sports Med. 2008 Jun;36(6):1160-3. “Topical glyceryl trinitrate significantly reduced pain with activity and at night, improved functional measures, and improved outcomes in patients with Achilles tendinopathy.”
- Paoloni JA, Murrell GA. Three-year followup of topical glyceryl trinitrate treatment of chronic noninsertional Achilles tendinopathy. Foot Ankle Int. 2007 Oct;28(10):1064-8.
- Paoloni JA, Murrell GA. Three-year followup of topical glyceryl trinitrate treatment of chronic noninsertional Achilles tendinopathy. Foot Ankle Int. 2007 Oct;28(10):1064-8. “Topical glyceryl trinitrate treatment has demonstrated efficacy in treating chronic noninsertional Achilles tendinopathy, and the treatment benefits continue at 3 years. Significant differences in asymptomatic patient outcomes for the glyceryl trinitrate group continue at 3 years, and this is confirmed by the effect size estimate. This suggests that the mechanism of action of topical glyceryl trinitrate on chronic tendinopathies is more than an analgesic effect.”
- Ohberg L, Alfredson H. Ultrasound guided sclerosis of neovessels in painful chronic Achilles tendinosis: pilot study of a new treatment. Br J Sports Med. 2002 Jun;36(3):173-5. “Sclerosing neovessels appears to be an effective treatment for painful chronic Achilles tendinosis, suggesting that neovessels play a key part in causing chronic tendon pain.”
- Alfredson H, Ohberg L. Sclerosing injections to areas of neo-vascularisation reduce pain in chronic Achilles tendinopathy: a double-blind randomised controlled trial. Knee Surg Sports Traumatol Arthrosc. 2005 May;13(4):338-44. “After completion of the study, treatment with Polidocanol injections (Cross-over in group B and additional treatments in group A) resulted in 10/10 and 9/10 satisfied patients in group A and B, respectively. In summary, injections with the sclerosing substance Polidocanol have the potential to reduce tendon pain during activity in patients with chronic painful mid-portion Achilles tendinopathy.”
- Lind B, Ohberg L, Alfredson H. Sclerosing polidocanol injections in mid-portion Achilles tendinosis: remaining good clinical results and decreased tendon thickness at 2-year follow-up. Knee Surg Sports Traumatol Arthrosc. 2006 Dec;14(12):1327-32. “treatment with sclerosing polidocanol injections in patients with chronic painful mid-portion Achilles tendinosis showed remaining good clinical results at a 2-year follow-up.”
- van Sterkenburg MN, et al. Less promising results with sclerosing ethoxysclerol injections for midportion achilles tendinopathy: a retrospective study. Am J Sports Med. 2010 Nov;38(11):2226-32. “Our study did not confirm the high beneficial value of sclerosing neovascularization in patients with midportion Achilles tendinopathy. Despite the retrospective design of our study, we consider it important to stress that injection of Ethoxysclerol may not be as promising as was thought.”
- van Sterkenburg MN, et al. Less promising results with sclerosing ethoxysclerol injections for midportion achilles tendinopathy: a retrospective study. Am J Sports Med. 2010 Nov;38(11):2226-32. “Our study did not confirm the high beneficial value of sclerosing neovascularization in patients with midportion Achilles tendinopathy. Despite the retrospective design of our study, we consider it important to stress that injection of Ethoxysclerol may not be as promising as was thought.”
- Ryan M, Wong A, Taunton J. Favorable Outcomes After Sonographically Guided Intratendinous Injection of Hyperosmolar Dextrose for Chronic Insertional and Midportion Achilles Tendinosis. AJR 2010;194:1047-53. “Dextrose injections appear to present a low-cost and safe treatment alternative with good long-term evidence for reducing pain from pathology at either the insertion or midportion of the Achilles tendon.“
- Yelland JM, et al. Prolotherapy injections and eccentric loading exercises for painful Achilles tendinosis: a randomised trial. Br J Sports Med. 2011 Apr;45(5):421-8. “For Achilles tendinosis, prolotherapy and particularly ELE combined with prolotherapy give more rapid improvements in symptoms than ELE alone but long-term VISA-A scores are similar.”
- Meakins, A. (2015, October 29). Prolotherapy… Is it as ‘sweet’ as it sounds??? Retrieved December 5, 2015, from https://thesportsphysio.wordpress.com/2012/11/20/prolotherapy-is-it-as-sweet-as-it-sounds/
- Rabago D, Slattengren A, Zgierska A. Prolotherapy in Primary Care Practice. Prim Care. 2010 Mar;37(1):65-80.
- Andres M, Murrell G. Treatment of Tendinopathy: What works, what does not, and what is on the horizon. Clin Orthop Relat Res. 2008 Jul;466(7):1539-54.”Current data support the use of eccentric strengthening protocols, sclerotherapy, and nitric oxide patches, but larger, multicenter trials are needed to confirm the early results with these treatments. Preliminary work with growth factors and stem cells is promising, but further study is required in these fields. Surgery remains the last option due to the morbidity and inconsistent outcomes. The ideal treatment for tendinopathy remains unclear.”
- de Vos RJ, et al. Platelet-rich plasma injection for chronic Achilles tendinopathy: a randomized controlled trial. JAMA. 2010 Jan 13;303(2):144-9. “Among patients with chronic Achilles tendinopathy who were treated with eccentric exercises, a PRP injection compared with a saline injection did not result in greater improvement in pain and activity.”
- Tsikopoulos K, et al. The clinical impact of platelet-rich plasma on tendinopathy compared to placebo or dry needling injections: A meta-analysis. Phys Ther in Sport. Jan 2016.17:87-94.
- Yee Lui PP. Stem cell technology for tendon regeneration: current status, challenges, and future research directions. Stem Cells Cloning. 2015;8:163-174. “the advantages and limitations of using different types of stem cells compared to terminally differentiated cells for tendon tissue engineering. The safety and efficacy of application of stem cells and their modified counterparts for tendon tissue engineering were then summarized after a systematic literature search in PubMed. The challenges and future research directions to enhance, optimize, and standardize stem cell-based therapies for augmenting tendon repair were then discussed.”
- Testa V, et al. Management of Achilles tendinopathy by ultrasound-guided percutaneous tenotomy. Med Sci in Sports Exerc. 2002, 34(40):573-580. “Percutaneous longitudinal ultrasound-guided internal tenotomy is simple, can be performed on an outpatient basis, requires minimal follow-up care, does not hinder further surgery should it be unsuccessful, and, in our experience, has produced no significant complications. It should be considered in the management of chronic Achilles tendinopathy after failure of conservative management. However, patients should be advised that, if they suffer from diffuse or multinodular tendinopathy or from pantendinopathy, a formal surgical exploration with stripping of the paratenon and multiple longitudinal tenotomies may be preferable.”
- Alfredson H, Cook J. A treatment algorithm for managing Achilles tendinopathy: new treatment options. Br J Sports Med. 2007 Apr;41(4):211-216. “Percutaneous tenotomy resulted in 75% of patients reporting good or excellent results after 18 months.“
- Andres M, Murrell G. Treatment of Tendinopathy: What works, what does not, and what is on the horizon. Clin Orthop Relat Res. 2008 Jul;466(7):1539-54. “Many studies evaluate various forms of surgery to treat Achilles tendinopathy…The results vary between studies and appear to correlate with the extent of tendon damage.”
- Morberg P. Long-term results after surgical management of partial Achilles tendon ruptures. Scand J Med Sci Sports. 1997 Oct;7(5):299-303. The conclusion of this study is that partial Achilles tendon ruptures are often difficult to treat and only two out of three patients can be expected to obtain satisfactory results after surgical treatment.”
- Paavola M, et al. Surgical treatment for chronic Achilles tendinopathy: a prospective seen month follow up study. Br J Sports Med. 2202 June;36(3):178-82. “Surgical treatment of chronic Achilles tendinopathy gives good and acceptable short term results. A lower complication rate and a trend to better recovery was observed in patients with peritendinous adhesions only than in those with peritendinous adhesions combined with an intratendinous lesion.”
- Khan W, et al. Analysing the outcome of surgery for chronic Achilles tendinopathy over the last 50 years. World J Orthop. 2015 Jul 18;6(6):491-497. “We conclude that although the success rate of surgery for chronic Acilles tendinopathy described in the literature has fallen over the last 50 years, this is probably due to a more rigorous methodology of the studies.”
- Tallon C, et al. Outcome of surgery for chronic Achilles tendinopathy. A critical review. Am J Sports Med. 2001 May-Jun;29(3):315-20. “Achilles tendinopathy is often treated surgically after failure of nonoperative management, but results are not uniformly excellent…..Study methods may influence reported surgical outcome, and we suggest guidelines for improving study design in this area of clinical research. We acknowledge that study methods have improved over the course of the past 20 years.”


Leave a Reply
Want to join the discussion?Feel free to contribute!