
AC Joint
The Acromioclavicular (AC) joint is the connection between your collarbone (clavicle) and shoulder blade (scapula) – the only boney attachment between your arm and your trunk.
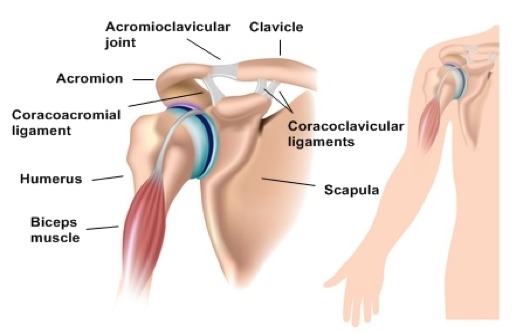
The proper functioning of this joint is necessary to ensure good shoulder mechanics and coordination of the scapula – especially with overhead motions. 1 2 3
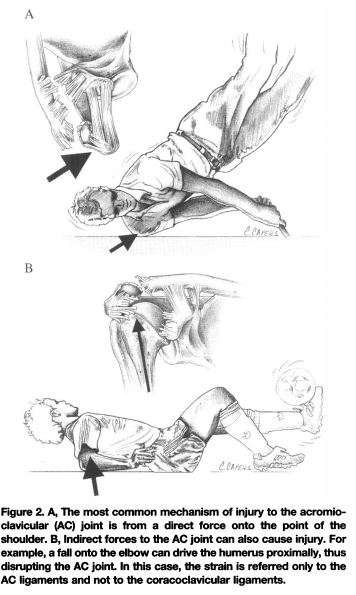
A traumatic AC joint injury is commonly referred to as a “Seperated Shoulder”. This injury occurs from direct downward impact to the acromion through a direct blow – as in a football tackle when the player is driven down onto their shoulder, or a slip and fall on your side with your arm tucked in by your side.
Collision sports, not surprisingly, have the highest rates of AC joint sprain. One study demonstrated a 45% incidence among professional rugby players (BTW – almost all ‘did well’ with conservative care). 4 Our sports physical therapists see these frequently with contact sports such as football, hockey, and lacrosse, as well as with skiers and cyclists who may crash and land on their shoulder.

X-rays can be helpful if a clavicle fracture is suspected, or in cases of complete displacement of the clavicle as in a type IV > VI (See grading system below). In these cases an MRI will often be ordered to visualize associated soft tissue damage. However, in most common cases (Grade I>II) imaging is not necessary as a diagnosis can be made based on the mechanism of injury and specific tests which can be done in the clinic.
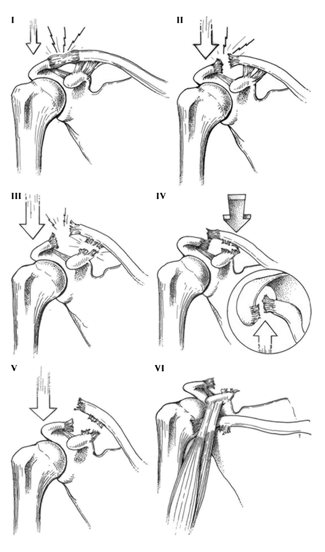
AC joint injuries are commonly ‘graded’ by severity:
Grade 1– Sprain of the acromioclavicular ligament
Grade 2– Tear of the acromioclavicular ligament, sprain of the corococlavicular ligament
Grade 3– Tear of acromioclavicular, corococlavicular ligaments, as well as the surrounding muscle and fascia.
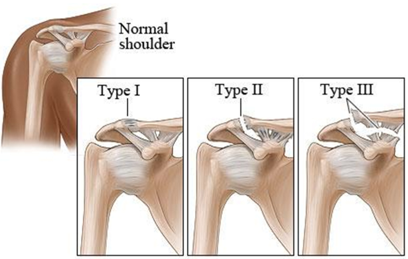
Classification of AC joint injuries can go further to include 6 ‘Types’. This is also based on severity with Type I > III being the same as above; Types VI > XI provide extra detail on more severe Grade III injuries with additional soft tissue damage surrounding the joint. The extensive damage described in types VI > XI are less common in typical sports injury – we see this type of trauma more commonly associated with a high impact or motor vehicle accident.5 6 7
What to do?
If you experience a Separated shoulder get evaluated by a trained medical professional. In cases where a clavicular fracture is suspected (or possible) X-rays will be necessary. Additionally, a systematic ‘check up’ of the athlete is indicated to rule out associated injuries such as a Rotator Cuff Injury or a Pneumothorax. While awaiting an evaluation the athlete should place the arm in a simple sling (available at most pharmacies). If tolerated, application of ice is wise for the first 2-3 days – typically 10-15 minutes every hour.
If the athlete experiences severe pain, obvious/severe deformity, shooting pains into the arm or neck, numbness/loss of sensation, shortness of breath, rapid breathing or other signs of physical distress, they should seek urgent medical attention.
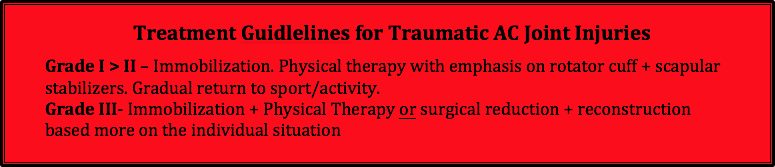
Grade 1-2 injuries do not require surgery – they are typically managed simply with Physical Therapy. 9 10 11
Treatment may include a brief period of immobilization with a sling – typically lasting as little as a few days, and up to a couple of weeks depending on severity of the injury. Once pain and swelling is under control it is important to begin a targeted rehab program that addresses range of motion and strength – with particular focus on the Serratus Anterior, Anterior Deltoid, and Trapezius Muscles which help to provide ‘dynamic stabilization’ to the AC joint. Abnormal scapular mechanics, referred to as scapular dyskensis, can occur if these muscles are not strengthened and retrained properly. It is believed that this could lead to secondary difficulties down the road in the improperly or incompletely rehabbed shoulder.
Additionally, the athlete will need to ‘re-mobilize’ surrounding joints. After an AC Joint injury and subsequent immobilization, often the Sternoclavicular Joint, Glenohumeral Joint, Scapulothoracic ‘Joint’, as well as the Spine (Neck>Thoracic Spine>Rib Cage) will experience some stiffness. Returning these structures to full mobility is essential, especially in the high performance athlete.
Most athletes can return to sport from a Grade I injury in 1-2 weeks.
Athletes with a Grade II should expect a 2-4 week period before initial return to sports activities. * Disclaimer! This is highly variable depending on a number of individual factors and sport-specific considerations.
The recommended management of Grade 3 injuries is more variable. There may be less pain than in a Grade II injury, despite a more obvious/severe deformity, as the ends of the involved bones are so displaced that little contact and/or rubbing takes place between them.12
There are arguments to support both operative and non-operative management of Grade III injuries; however, a recent systematic review of the best available research reported comparable results when considering pain, motion, strength, and function. 13 14 15 16 There are several factors that are worth considering when deciding the best management for these injuries.
- Risk – not surprisingly there is a much higher (although still small) risk associated with surgical management compared to conservative including. Reported complications from surgery include infection, pin migration, keloid scarring, visual deformity and post-operative stiffness. 17 18
- Functional level – The literature suggests that individuals looking to return to a high level of activity (throwing/overhead athletes or overhead workers) may have better outcomes with surgical intervention. 19 20
- Cost – Surgical management (surgery + Post-op physical therapy) would be significantly more expensive than physical therapy alone. 21 22
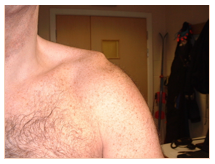
- Cosmetic – Shoulder separation do not reduce on there own. This likely means that there will be a visual deformity that is always present. 23 24
* There are multiple ‘worn’ devices on the market designed to ‘reduce the deformity’. These are almost always quite uncomfortable and have been associated with skin breakdown and necrosis. What’s more, the research has demonstrated no improvement associated with these devices when compared to ‘skillful neglect’.25 They should be avoided.
What does the surgical reduction & reconstruction look like?
See the following videos for a nice animated video of 2 common approaches.
https://www.youtube.com/watch?v=kpazACvnkj4
https://www.youtube.com/watch?v=LerMY0XpKE4
When can I return to my sport?
In general traumatic AC joint injuries recover quite well. There is no concrete timeline and it is largely based on the individual injury and the demands of the sports.
In general, Grade I injuries should expect 1-2 weeks before initiating a graded return to sporting activity. Grade II 2-4 weeks (Variable). Grade III 4-12 weeks (Highly Variable).
At VASTA we have a specific evidence-based return to sport testing for the shoulder to help us make the best decision of when it is appropriate to return to your sport. Our goal is to get you better, faster.
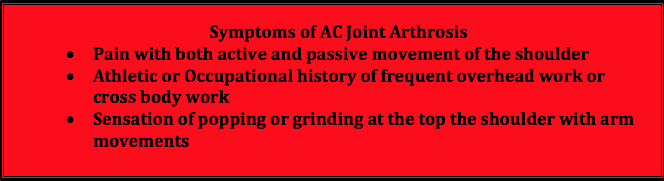
Other Mechanisms of AC Joint Pain
Non-Traumatic AC joint injury
Pain at the top of the shoulder, over the AC joint is also possible even without a traumatic mechanism of injury. The disc that provides cushion to the joint surfaces eventually wears as we age- and it’s been shown that this process starts when we are in our twenties! 26 27 In addition to aging, repetitive micro-trauma (think overhead workers or athletes) and chronic joint instability (which may be the result of previous AC joint sprain) can expedite degenerative changes. 28
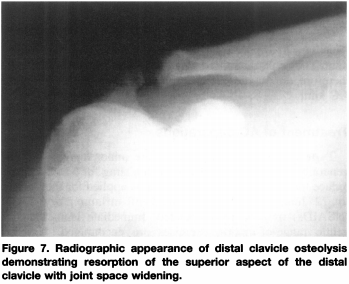
Osteolysis of the AC Joint is another cause of AC joint breakdown common in weightlifters. Heavy weight training places large compressive loads across the AC joint. Additionally, poor form leads to excessive shearing strains to the joint. ‘Weightlifters Osteolysis’ is thought to be caused by repetitive microtrauma leading to stress fractures at the ends of the bones at the AC joint.29 The bone then experiences a reduction of local blood supply and undergoes a process of bone resorption, leading to a widening of the joint space and a loss of stability.
Unfortunately physical therapy does not seem to be as beneficial in case of severe joint degeneration. Physical therapy can help to improve ROM, strength and function, but often has little effect on pain without activity modification. 30 31
Injections have also been proposed and can be beneficial for short-term pain relief, but this is temporary relief and does not alter the disease progression.32
For those who do not get benefit from conservative treatment, surgical treatment may be indicated. A distal clavical excision (DCE) is typically performed and involves removing the lateral 6-7mm of bone at the end of the collarbone. This minimizes the bone-to-bone contact at the AC joint with overhead reaching.

This procedure can be done both arthroscopically or as an “’open” procedure, with both having reported very favorable long-term outcomes. 33 34
AC joint degeneration rarely happens in isolation – there is frequently rotator cuff damage, labral (cartilage) fraying, and/or secondary impingement, which should also be addressed. A thorough clinical exam is crucial to accurate diagnosis and to identify all of factors that are contributing to pain.35
If you are ‘dealing’ with an acute or long-standing AC joint issue – see your trusted Sports Physical Therapist!
- Xinning Li, MD; Richard Ma, MD; Asheesh Bedi, MD; David M. Dines, MD; David W. Altchek, MD; Joshua S. Dines, MD. Current Concepts Review Management of Acromioclavicular Joint Injuries. J Bone Joint Surg Am, 2014 Jan 01; 96 (1): 73 -84. “Acromioclavicular joint injuries are common shoulder injuries that often result from direct trauma sustained during participation in contact sports. Anterior-to-posterior stability is provided by the acromioclavicular ligaments, while superior stability is provided by the coracoclavicular ligaments.”
- Spencer EE Jr. Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007 Feb;455(Feb):38-44. “The three prospective, randomised studies all concluded that non-operative treatment was superior to surgery. Outcomes after surgery were no better than after non-surgical treatment, and surgery was associated with more complications, increased convalescence, and longer time away from work and sport.”
- Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr. Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med. 2013;41(22):2684-2692. “Osteoarthritis of the acromioclavicular (AC) joint is a common condition causing anterior or superior shoulder pain, especially with overhead and cross-body activities.”
- Beim G. Acromioclavicular Joint Injuries. Journal of Athletic Training 2000;35(3):261–267 “…The most common events associated with AC injuries include contact sports such as hockey, rugby, and football. Webb and Bannister’4 noted a 45% incidence of AC injuries in first-class rugby players, and most did well with conservative treatment.”
- Xinning Li, MD; Richard Ma, MD; Asheesh Bedi, MD; David M. Dines, MD; David W. Altchek, MD; Joshua S. Dines, MD. Current Concepts Review Management of Acromioclavicular Joint Injuries. J Bone Joint Surg Am, 2014 Jan 01; 96 (1): 73 -84. “Acromioclavicular joint injuries are among the most common shoulder girdle injuries in athletes and most commonly result from a direct force to the acromion with the arm in an adducted position.”
- Spencer EE Jr. Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007 Feb;455(Feb):38-44. “This review compared the efficacy of operative and non-operative treatment of grade III acromioclavicular separations. The author concluded that limited evidence suggests that non-operative treatments are superior. “
- Korsten K, Gunning AC, Leenen LPH. Operative or conservative treatment in patients with Rockwood type III acromioclavicular dislocation: a systematic review and update of current literature. International Orthopaedics. 2014;38(4):831-838. doi:10.1007/s00264-013-2143-7. “The objective and subjective shoulder function outcome was better in the operative group, especially in young adults, though the rate of complications and radiographic abnormalities were higher. The rehabilitation time was shorter in the conservative group, however the cosmetic outcome was worse.”
- Johnson L, Polson K, Reid D. Acromioclavicular joint separations grade I-III: best practice guidelines. Auckland: New Zealand Academy of Sport, 2011: 1-54. 8Johnson L, Polson K, Reid D. Acromioclavicular joint separations grade I-III: best practice guidelines. Auckland: New Zealand Academy of Sport, 2011: 1-54. “Historically, most studies have reported satisfactory results after nonoperative treatment for those with type I and II injuries”
- Xinning Li, MD; Richard Ma, MD; Asheesh Bedi, MD; David M. Dines, MD; David W. Altchek, MD; Joshua S. Dines, MD. Current Concepts Review Management of Acromioclavicular Joint Injuries. J Bone Joint Surg Am, 2014 Jan 01; 96 (1): 73 -84. “Type-I or type-II acromioclavicular joint injuries have been treated with sling immobilization, early shoulder motion, and physical therapy, with favorable outcomes.”
- Mikek M. Long-term shoulder function after type I and II acromioclavicular joint disruption. Am J Sports Med. 2008 Nov;36(11):2147-50. “Acromioclavicular joint separations are very common lesions, with the majority falling into Rockwood classification type I and II. It is generally agreed that conservative treatment of these injuries leads to good functional results, although there are some studies that suggest these injuries are associated with a high incidence of persistent symptoms.”
- Beim G. Acromioclavicular Joint Injuries. Journal of Athletic Training 2000;35(3):261–267 “…The most common events associated with AC injuries include contact sports such as hockey, rugby, and football. Webb and Bannister’4 noted a 45% incidence of AC injuries in first-class rugby players, and most did well with conservative treatment.”
- Johnson L, Polson K, Reid D. Acromioclavicular joint separations grade I-III: best practice guidelines. Auckland: New Zealand Academy of Sport, 2011: 1-54. “Historically, most studies have reported satisfactory results after nonoperative treatment for those with type I and II injuries”
- Xinning Li, MD; Richard Ma, MD; Asheesh Bedi, MD; David M. Dines, MD; David W. Altchek, MD; Joshua S. Dines, MD. Current Concepts Review Management of Acromioclavicular Joint Injuries. J Bone Joint Surg Am, 2014 Jan 01; 96 (1): 73 -84. “Type-I or type-II acromioclavicular joint injuries have been treated with sling immobilization, early shoulder motion, and physical therapy, with favorable outcomes.”
- Spencer EE Jr. Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007 Feb;455(Feb):38-44. “This review compared the efficacy of operative and non-operative treatment of grade III acromioclavicular separations. The author concluded that limited evidence suggests that non-operative treatments are superior. “
- Gstettner C, Tauber M, Hitzl W, Resch H. Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):220-5.” The best treatment for Rockwood type III injries is still controversial….24 patients who were treated surgically with a hook plate and 17 conservatively treated patients were examined iwht a mean follow-up of 34 months….In this study, better results were achieved by surgical treatment with the hook plate than by conservative treatment.”
- Spencer EE Jr. Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007 Feb;455(Feb):38-44. “This review compared the efficacy of operative and non-operative treatment of grade III acromioclavicular separations. The author concluded that limited evidence suggests that non-operative treatments are superior. “
- Gstettner C, Tauber M, Hitzl W, Resch H. Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):220-5.” The best treatment for Rockwood type III injries is still controversial….24 patients who were treated surgically with a hook plate and 17 conservatively treated patients were examined iwht a mean follow-up of 34 months….In this study, better results were achieved by surgical treatment with the hook plate than by conservative treatment.”
- Spencer EE Jr. Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007 Feb;455(Feb):38-44. “This review compared the efficacy of operative and non-operative treatment of grade III acromioclavicular separations. The author concluded that limited evidence suggests that non-operative treatments are superior. “
- Gstettner C, Tauber M, Hitzl W, Resch H. Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):220-5.” The best treatment for Rockwood type III injries is still controversial….24 patients who were treated surgically with a hook plate and 17 conservatively treated patients were examined iwht a mean follow-up of 34 months….In this study, better results were achieved by surgical treatment with the hook plate than by conservative treatment.”
- Spencer EE Jr. Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007 Feb;455(Feb):38-44. “This review compared the efficacy of operative and non-operative treatment of grade III acromioclavicular separations. The author concluded that limited evidence suggests that non-operative treatments are superior. “
- Gstettner C, Tauber M, Hitzl W, Resch H. Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):220-5.” The best treatment for Rockwood type III injries is still controversial….24 patients who were treated surgically with a hook plate and 17 conservatively treated patients were examined iwht a mean follow-up of 34 months….In this study, better results were achieved by surgical treatment with the hook plate than by conservative treatment.”
- Spencer EE Jr. Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007 Feb;455(Feb):38-44. “This review compared the efficacy of operative and non-operative treatment of grade III acromioclavicular separations. The author concluded that limited evidence suggests that non-operative treatments are superior. “
- Gstettner C, Tauber M, Hitzl W, Resch H. Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):220-5.” The best treatment for Rockwood type III injries is still controversial….24 patients who were treated surgically with a hook plate and 17 conservatively treated patients were examined iwht a mean follow-up of 34 months….In this study, better results were achieved by surgical treatment with the hook plate than by conservative treatment.”
- Beim G. Acromioclavicular Joint Injuries. Journal of Athletic Training 2000;35(3):261–267 “…The most common events associated with AC injuries include contact sports such as hockey, rugby, and football. Webb and Bannister’4 noted a 45% incidence of AC injuries in first-class rugby players, and most did well with conservative treatment.”
- Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr. Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med. 2013;41(22):2684-2692. “Osteoarthritis of the acromioclavicular (AC) joint is a common condition causing anterior or superior shoulder pain, especially with overhead and cross-body activities.”
- Lervick GN. Direct Arthroscopic Distal Clavicle Resection: A Technical Review. The Iowa Orthopaedic Journal. 2005;25:149-156. “Treatment of isolated AC joint osteoarthritis is initially non-surgical. When such treatment fails to provide lasting relief, surgical treatment is warranted. Direct (superior) arthroscopic resection of the distal (lateral) end of the clavicle is a successful method of treating the condition, as well as other isolated conditions of the AC joint.”
- Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr. Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med. 2013;41(22):2684-2692. “Osteoarthritis of the acromioclavicular (AC) joint is a common condition causing anterior or superior shoulder pain, especially with overhead and cross-body activities.”
- Beim G. Acromioclavicular Joint Injuries. Journal of Athletic Training 2000;35(3):261–267 “…The most common events associated with AC injuries include contact sports such as hockey, rugby, and football. Webb and Bannister’4 noted a 45% incidence of AC injuries in first-class rugby players, and most did well with conservative treatment.”
- Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr. Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med. 2013;41(22):2684-2692. “Osteoarthritis of the acromioclavicular (AC) joint is a common condition causing anterior or superior shoulder pain, especially with overhead and cross-body activities.”
- Lervick GN. Direct Arthroscopic Distal Clavicle Resection: A Technical Review. The Iowa Orthopaedic Journal. 2005;25:149-156. “Treatment of isolated AC joint osteoarthritis is initially non-surgical. When such treatment fails to provide lasting relief, surgical treatment is warranted. Direct (superior) arthroscopic resection of the distal (lateral) end of the clavicle is a successful method of treating the condition, as well as other isolated conditions of the AC joint.”
- Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr. Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med. 2013;41(22):2684-2692. “Osteoarthritis of the acromioclavicular (AC) joint is a common condition causing anterior or superior shoulder pain, especially with overhead and cross-body activities.”
- Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr. Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med. 2013;41(22):2684-2692. “Osteoarthritis of the acromioclavicular (AC) joint is a common condition causing anterior or superior shoulder pain, especially with overhead and cross-body activities.”
- Lervick GN. Direct Arthroscopic Distal Clavicle Resection: A Technical Review. The Iowa Orthopaedic Journal. 2005;25:149-156. “Treatment of isolated AC joint osteoarthritis is initially non-surgical. When such treatment fails to provide lasting relief, surgical treatment is warranted. Direct (superior) arthroscopic resection of the distal (lateral) end of the clavicle is a successful method of treating the condition, as well as other isolated conditions of the AC joint.”
- Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr. Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med. 2013;41(22):2684-2692. “Osteoarthritis of the acromioclavicular (AC) joint is a common condition causing anterior or superior shoulder pain, especially with overhead and cross-body activities.”


Share this entry