BLOOD FLOW RESTRICTION TRAINING
At VASTA, we are naturally skeptical of ‘new’ treatment approaches, especially those that make BIG promises. Our clinicians are current with best practices and are committed to an evidence-based approach.
At the same time, we work hard to stay on the cutting edge of emerging treatment techniques.
Blood Flow Restriction (BFR) Training is one such approach.
Recently, this little known technique has become a popular tool at military hospitals for soldiers who experienced significant limb trauma (e.g. in ‘limb salvage’ wards) and with amputees. Millions of dollars of research has been poured into exploring the utility of BFR for patients with significant limitations (i.e. limited mobility and/or limited ability to bear weight) who need to build muscle. A very difficult task!
Similarly, our patients with post-operative limitation that prohibits weight bearing or heavy use of the LE for weeks (or even months) end up with dramatic muscle atrophy. Previously thought of as a ‘necessary evil’ to protect the surgical repair… Now, maybe not!
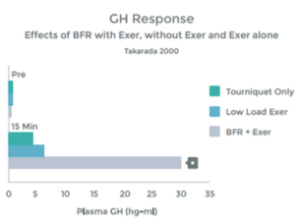
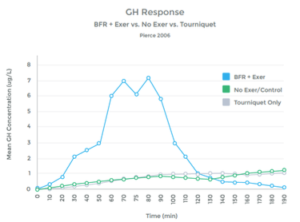
BFR involves restricting the blood flow to a limb during exercise in order to starve the muscle of oxygen, thus causing a number of ‘pro-growth’ chemical and hormonal changes. This allows us to stimulate muscle hypertrophy (growth) with very low intensity & low load exercises.
For any patient requiring a prolonged period of ‘rest’, immobilization or limited weight bearing – we believe BFR training has the potential to be a game changer.
What is Blood Flow Restriction Training?
Blood flow to the limb is significantly reduced, and blood return (flow out of the limb) is completely stopped, for a brief period of time, with the use of a tourniquet. This specially designed tourniquet contains a Doppler (to sense blood flow) and is automated to control blood flow to precisely defined parameters.
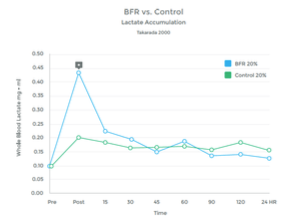
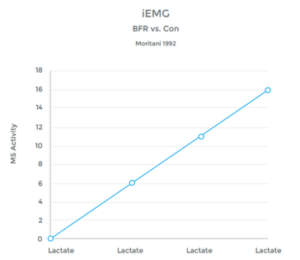
Once blood flow is reduced to the limb, the patient performs ~ 4-5 minutes of low intensity resistance training (LIT) exercises. While the load is very light – and thus the strain to the bone, cartilage, ligaments, etc. is minimal – the muscle gets exhausted! This is because it is being forced to work under anaerobic conditioning (without oxygen from fresh blood supply). Thus, the muscle seems to work very hard, all muscle fiber types are recruited, lactic acid builds up, the muscle glycogen levels become depleted and the exerciser feels as though they have just worked out really hard.
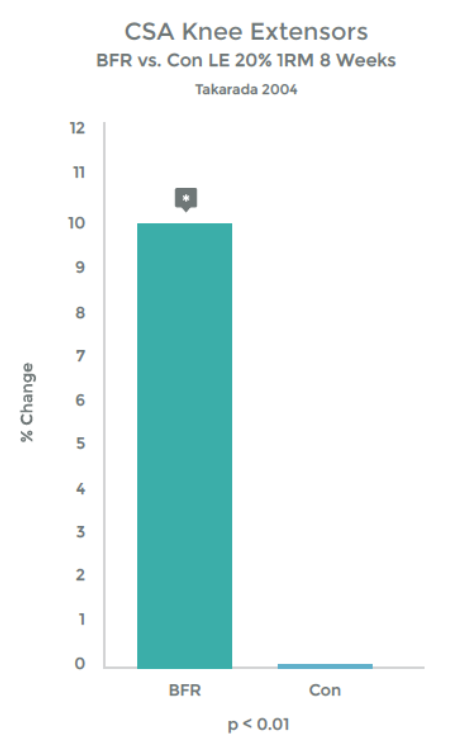
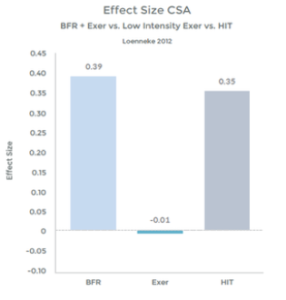
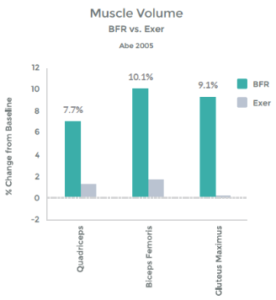
More importantly, the muscle also thinks it worked out really hard; and, the response is similar to high intensity training (HIT) – The muscle grows and gets stronger!
Bottom line – this technology allows us to achieve strength and hypertrophy (size) gains that, under normal circumstances, are possible only under high loads & high exercise intensities.
We can make gains earlier and faster, even when an injury prevents you from exercising.
For an example of it’s sport-specific use, check out this blog by our very good friends at Union PT in Seattle! https://www.unionpt.com/getting-back-on-the-rock-sooner/
For those looking for more detail and a review of the extensive research that has been done in this field, read on…