

What Is It?
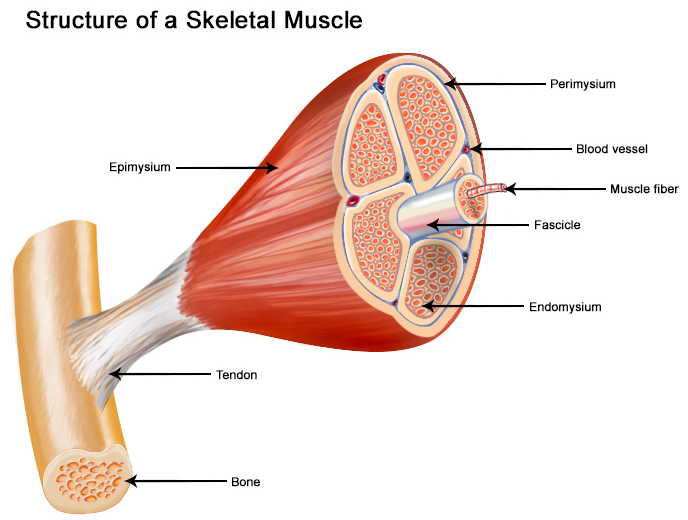
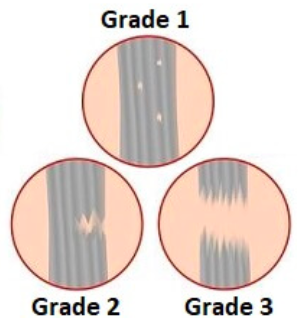
A muscle strain refers to a tear of the muscle. The severity of tearing can vary greatly. Strains are typically classified as either minor, moderate, or severe depending on the extent of tearing. Most readers may be familiar with a grading system that categorizes the tear (strain) according to the % of the muscle disrupted. Remember a muscle is really thousands of muscle fibers.

These definitions differ slightly from source to source, but typically are close to the following:
- Grade I – ‘Minor’ < 5% of total # of muscle fibers torn
- Grade II – ‘Moderate’ > 5%, but < 50% of total # of muscle fibers torn
- Grade III – Complete or Near Complete (Subtotal) tears. This includes an injury where the majority of the fibers are torn but the fascia surrounding the muscle remains intact to some degree. This category would also include a complete rupture, which is rare.

Often, the tear happens suddenly and is often unmistakable – athletes frequently report feeling as though they’ve been stabbed!


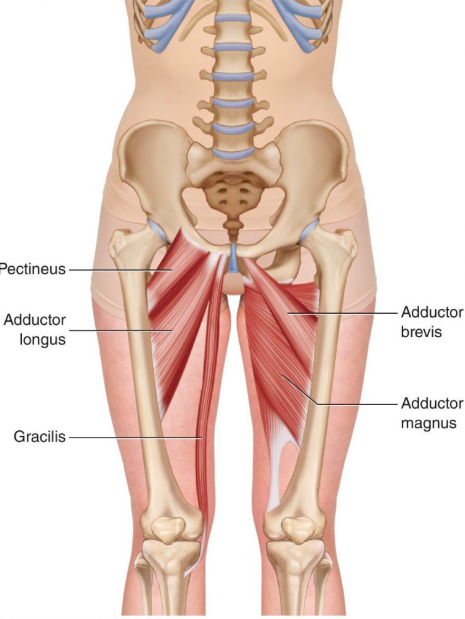
Groin injuries are most commonly seen among the athletic population. They frequently involve the adductor longus, along with 1 or more other muscles in the region.1 These muscles are localized within the inner thigh. Their primary role during running is to provide pelvic stability during the single-leg support phase. They also bring the femur towards midline and assist in forward and backward motion of the leg during your stride.2

Mechanism of Injury
A Groin strain primarily occurs when there is a sudden explosive change in direction Particularly with lateral movement). Accelerating in sprinting is another potential mechanism of injury, along with jumping and overstretching the groin tendons. 13
To put this into perspective, in 4 of the top English premier soccer leagues, hip and groin injuries account for 12% of all injuries.46 47Thorborg K, Reiman M, Weir A, Kemp J, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. JOSPT. 2018;48:239-249 48
Stretching may also be initiated in this stage, starting with ‘manual stretching’ (by your therapist) and progressing to self-stretching.
Manual therapy techniques to promote tissue mobility may also be initiated during this phase – this may include instrumented soft tissue mobilization, and active release techniques.
General conditioning exercise will limit deconditioning while you are recovering (Remember, these injuries tend to occur when the athlete is fatigued). Light agility activities that are specific to your sport can also be initiated.


Return to Sport Phase
When progressing to the final phase of recovery, a patient must demonstrate normalized hip range of motion when compared to the uninvolved leg. Their groin strength must be 75% of the uninvolved leg, and must be pain free. 49Thorborg K, Reiman M, Weir A, Kemp J, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. JOSPT. 2018;48:239-249 50 (As determined by your physical therapist through re-assessment)
At this point, heavier sport-specific training can be initiated. Agility work and general conditioning will continue to be progressed by increasing speed, power, and resistance.
This loading will be progressed to unstable surfaces, in unstable positions and throughout functional activities to mimic sport specific movement patterns.
Eccentric loading is also important to progress in this stage, as heavy eccentric loads must be tolerated prior to return to sport.
There is a lot of research indicating that ‘lengthened state’ strength (the ability of the muscle to effectively produce force near it’s end-range of stretch) is paramount for the high-demand, multi-directional athlete. Failure to normalize this is likely a significant contributor to the very high recurrence rates seen in some sports. 51Tyler T, Schmitt B, Nicholas S, McHugh M. Rehabilitation after hamstring-strain injury emphasizing eccentric strengthening at long muscle lengths: results of long-term follow up. J of Sport Rehab. 2016;26(2)131-40.52
If you plan to return to high risk sports (ice hockey, soccer, football) and you are pushing the time frame for return to sport, compression shorts can be utilized to potential reduce re-injury risk. 53Tyler T, Schmitt B, Nicholas S, McHugh M. Rehabilitation after hamstring-strain injury emphasizing eccentric strengthening at long muscle lengths: results of long-term follow up. J of Sport Rehab. 2016;26(2)131-40.54


For a successful return to sport, rehab must be completed.
As previously discussed, a previous groin strain puts you at much greater risk for another groin related injury. Completing rehab in its entirety can reduce recurrence risk. 55Kaariainen M, et al. Correlation between biomechanical and structural changes during the regeneration of skeletal muscle after laceration injury. J of Ortho Research. 1998; 16(2)197-2016.56
Make sure you complete your REHAB!!!
At VASTA Performance Training and Physical Therapy, our clinicians are Sports and Performance focused. By leveraging the best practices of Rehabilitative Medicine and Strength & Conditioning, we’ll get you back in the game, preforming better than before your injury!
Experience the VASTA Difference – Request an appt. or call us today to get started immediately. 802-399-2244.
- Renstrom P, Peterson L. Groin injuries in athletes. Brit J Sports Med. 1980;14:30-36
- Renstrom P, Peterson L. Groin injuries in athletes. Brit J Sports Med. 1980;14:30-36
- Kiel J, Kaiser K. Adductor Strain. [Updated 2018 Dec 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-.3
The musculotendinous junction (where muscle turns into tendon) of the adductor longus is the most common location for a strain.4 Thorborg K, Reiman M, Weir A, Kemp J, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. JOSPT. 2018;48:239-249 5 An acute adductor longus injury may also involve a tendinous rupture (usually close to the muscles insertion on the pelvis) or avulsion (when the tendon pulls a chunk of bone off the pelvis). 6Thorborg K, Reiman M, Weir A, Kemp J, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. JOSPT. 2018;48:239-249 7
Who Gets It?
Groin injuries are most common in male athletes who participate in multidirectional sports. They are especially prevalent in football, ice hockey and soccer. These sports often involve repetitive and explosive hip movements such as high intensity kicking, skating and direction changes. 8Thorborg K, Reiman M, Weir A, Kemp J, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. JOSPT. 2018;48:239-249 9
The biggest risk factor for suffering a groin strain is having a history of previous groin injury. One study demonstrated that 63% of all adductor strains occur in those who presented with prior adductor injuries. 10Schlegel T, Bushnell B, Godfrey J, Boublik M. Success of nonoperative management of adductor longus tendon rupture in national football league athletes. Am J Sports Med. 2009;37:1294-1399 11The preseason and late season are the most common points during a season in which groin strains happen, perhaps indicating insufficient off season conditioning, and/or late season fatigue. These injuries occur almost exclusively with sprinting, cutting, and max effort acceleration and deceleration.12Renstrom P, Peterson L. Groin injuries in athletes. Brit J Sports Med. 1980;14:30-36
- Werner J, Hagglund M, Walden M, Ekstrand J. UEFA injury study: a propesitve study of hip and groin injuries in professional football over seven consecutive seasons. Brit J Sports Med. 2009;13:1036-104014They are also commonly seen in the NFL with a reported annual incidence of between 5-28% of all injuries. 15Thorborg K, Reiman M, Weir A, Kemp J, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. JOSPT. 2018;48:239-249 16
How to Prevent it?
There are many risk factors that have been identified for a groin muscle injury:
- Age – The aging athlete is more prone to injury
If the ratio of adductor to abductor strength is less than 80%, athletes are 17x more likely to experience a groin strain. 17 Thorborg K, Reiman M, Weir A, Kemp J, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. JOSPT. 2018;48:239-249 18
- Flexibility – some studies show that impaired hip abduction as well as decreased total arc of hip rotation range of motion can be risk factors for groin strain. 19Tyler T, Nicholas S, Campbell R, McHugh M. The association of hip strength and flexibility with the incidence of adductor muscle strains in professional ice hockey players. Am J Sports Med. 2001;29:124-128 20
- Off Season Training – Limited off season training can result in increased adductor strain risk. 21Thorborg K, Reiman M, Weir A, Kemp J, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. JOSPT. 2018;48:239-249 22 Therefore, don’t go into your season cold!
- Prior Injury – By far the strongest risk factor is prior injury, specifically in soccer, football and ice hockey.23Engebretsen A, Myklebust G, Holme I, Bahr R. Intrinsic risk factors for groin injuries among male soccer players: a prospective cohort study. Am J Sports Med.2010;38:2051-205724 This highlights the importance of a full recovery prior to returning to sport. Overall, re-injury rates hover around 1/3 for most sports, with the greatest risk of re-injury occurring during the initial 2 weeks upon return to sport.25Orchard J, Seward H. Epidemiology of injuries in the Australian Football League, seasons 1997–2000. Brit J of Sports Med. 2002;36(1):39-4426
There are prevention programs that have been shown to be beneficial in reducing groin injury rates. A specific study that implemented a 2-year prevention program with the NY Islanders demonstrated a 78% decreased injury rate per 1000 player games. This program focused on hip adductor strengthening, eccentric training, and functional conditioning. 27Tyler T, Nicholas S, Campbell R, McHugh M. The association of hip strength and flexibility with the incidence of adductor muscle strains in professional ice hockey players. Am J Sports Med. 2001;29:124-128 28
For our high-demand athletes and/or high-risk recreational athletes we strongly recommend the following – Consult with a sports medicine specialist to develop a comprehensive pre-season training plan that incorporates sport-specific conditioning activities as well as an appropriate ‘balance’ of strengthening and mobility drills. Also, for those competing at high intensities, heavy eccentric adductor strengthening is a must.
*Seek the advice of a Sports Physical Therapist or Strength & Conditioning coach*What is my Prognosis?
Recovery from a groin strain can vary greatly among each individual – from 1 week to 6 months! However, there are a few factors that can be used to determine if an athlete will progress faster or slower than expected:
- Location – If the strain is closer to the pelvis (eg. ‘higher’), this may require more time for recovery as opposed to an injury that is located lower down the leg.29Heiderscheit BC, Sherry MA, Silder A, Chumanov ES, Thelen DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. J of Orthop & Sports Phys Ther. 2010;40(2):67-81.30
- Injury ‘Length’ – The length of palpable tenderness within the muscle is correlated to recovery time frame. If the strain is smaller in longitudinal length (the length of palpable pain along the muscle is small), then recovery is typically faster and vice versa. 31Heiderscheit BC, Sherry MA, Silder A, Chumanov ES, Thelen DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. J of Orthop & Sports Phys Ther. 2010;40(2):67-81.32
- Mechanism of injury – There are 2 primary mechanisms for tearing your adductor. 1) Stretch-Type Injury tend to recover slower and require extended periods of time away from sport. 2) Sprinting Injury, usually seen with explosive lateral movement. These may recover quicker than a stretch-type injury. 33Heiderscheit BC, Sherry MA, Silder A, Chumanov ES, Thelen DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. J of Orthop & Sports Phys Ther. 2010;40(2):67-81.34
- Initial recovery speed – Lastly, looking at an athlete’s early response to treatment can provide some insight on prognosis. If, during the first week of recovery they are responding well (e.g. pain levels are decreasing rapidly, gait is normalizing, range of motion is returning quickly and swelling/bruising has reduced) then the prognosis is better compared to an athlete who demonstrates minimal improvement in the initial 5-10 days.35Jacobsen P, Witvrouw E, Muxart P, Tol JL, Whiteley R. A combination of initial and follow-up physiotherapist examination predicts physician-determined time to return to play after hamstring injury, with no added value of MRI. Brit J of Sports Med. 2016;50(7):431-9.36
How do I approach treating it?
Acute Stage
Treatment can be initiated a few days after injury, depending on injury severity.
The first few days of treatment will include techniques to reduce excessive swelling, promote lymph drainage and manage pain. This can include soft tissue massage, modalities (electrical stimulation), and intermittent icing (every 15 minutes for the first 48 hours). If gait abnormalities are noted, crutches may be recommended by your physical therapist – avoiding limping is important, listen to this recommendation!
Complete rest is not recommended. After injury you will want to initiate low load and high repetition activities within the pain free range. Doing something is important, even if this is limited to very light isometric activation of the muscle (consult with a Sports Physical Therapist to determine what the right starting point is for you). Early initiation of treatment helps to stimulate cells to regenerate muscle fibers, and (importantly!) helps to prevent excessive scarring down of the new muscle tissue.37Jarvinen T, et al. Muscle Injuries. The Am J of Sports Med. 2005; 33(5)745-64.38 Last, early and appropriate muscle activation promotes proper alignment of new muscle fibers and improved circulation of the regenerating tissues,39Heiderscheit BC, Sherry MA, Silder A, Chumanov ES, Thelen DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. J of Orthop & Sports Phys Ther. 2010;40(2):67-81.40 laying the foundation for a healthy ‘bridge’ across the injury – imperative before progressing to the strengthening phase of rehabilitation.
Stretching is to be avoided for up to 14 days.41Kaariainen M, et al. Correlation between biomechanical and structural changes during the regeneration of skeletal muscle after laceration injury. J of Ortho Research. 1998; 16(2)197-2016.42
Stretching a muscle that is trying to heal can affect the scar formation and healing process. 43Jarvinen T, et al. Muscle Injuries. The Am J of Sports Med. 2005; 33(5)745-64.44
Ultimately, make sure you are remaining active without significant exacerbation of pain. You will work with your PT to find the right ‘dose’ of exercise.
Sub-Acute Stage
Phase 2 of healing incorporates progressive loading of the groin musculature. Isolated loads to the adductor will continue and progress. Also, diversifying movements is important during this stage. You will work towards heavier functional movement patterns such as sumo squats, split stance squats, lunges and slide board activities. You will start by working in small ranges and progressing to larger ranges of motion. We also want to make sure that your hip and core control is strong and coordinated.
Focused “Eccentric” exercises to the adductors will be introduced (this includes loading the muscles while they are being lengthened).45Renstrom P, Peterson L. Groin injuries in athletes. Brit J Sports Med. 1980;14:30-36